Publication
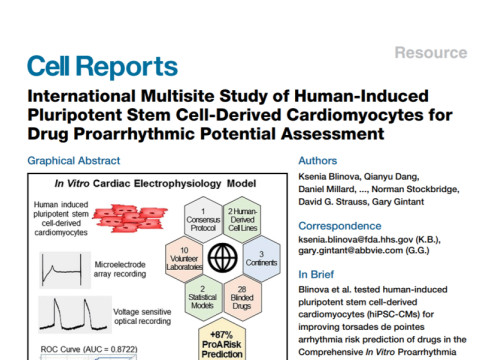
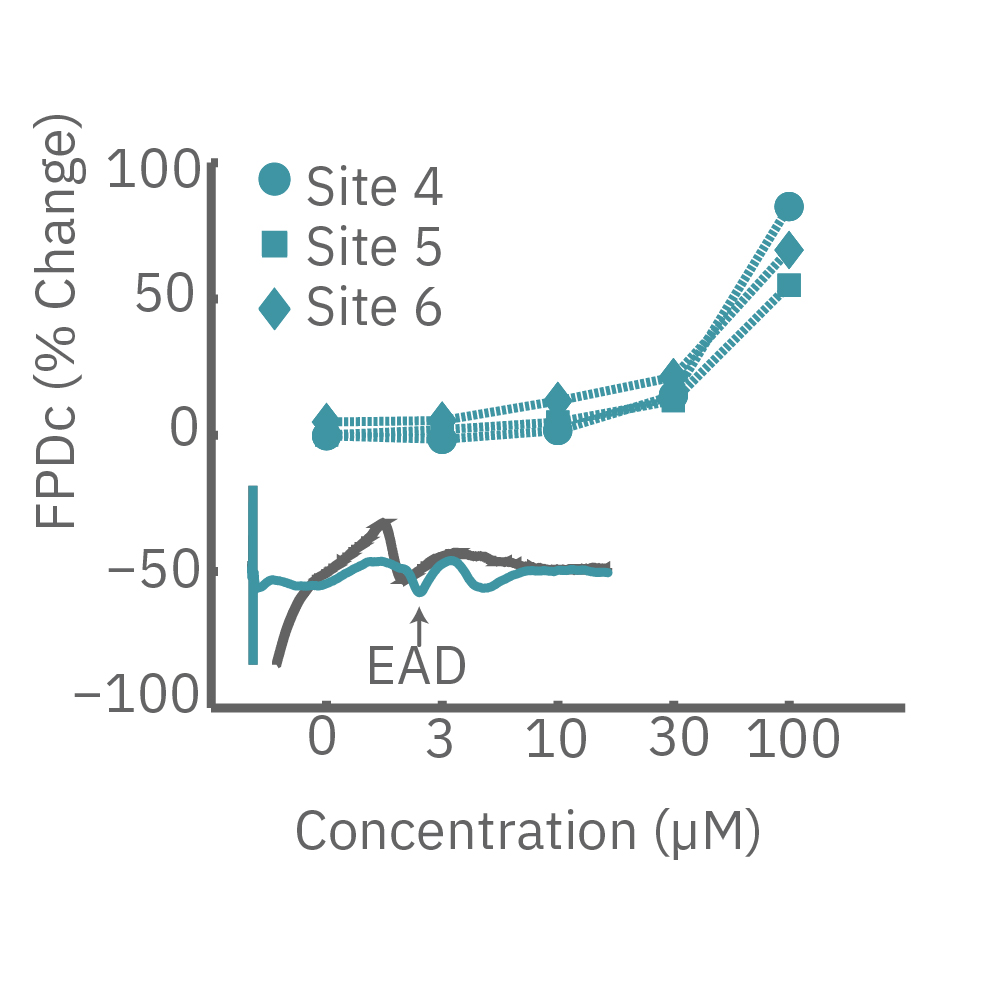
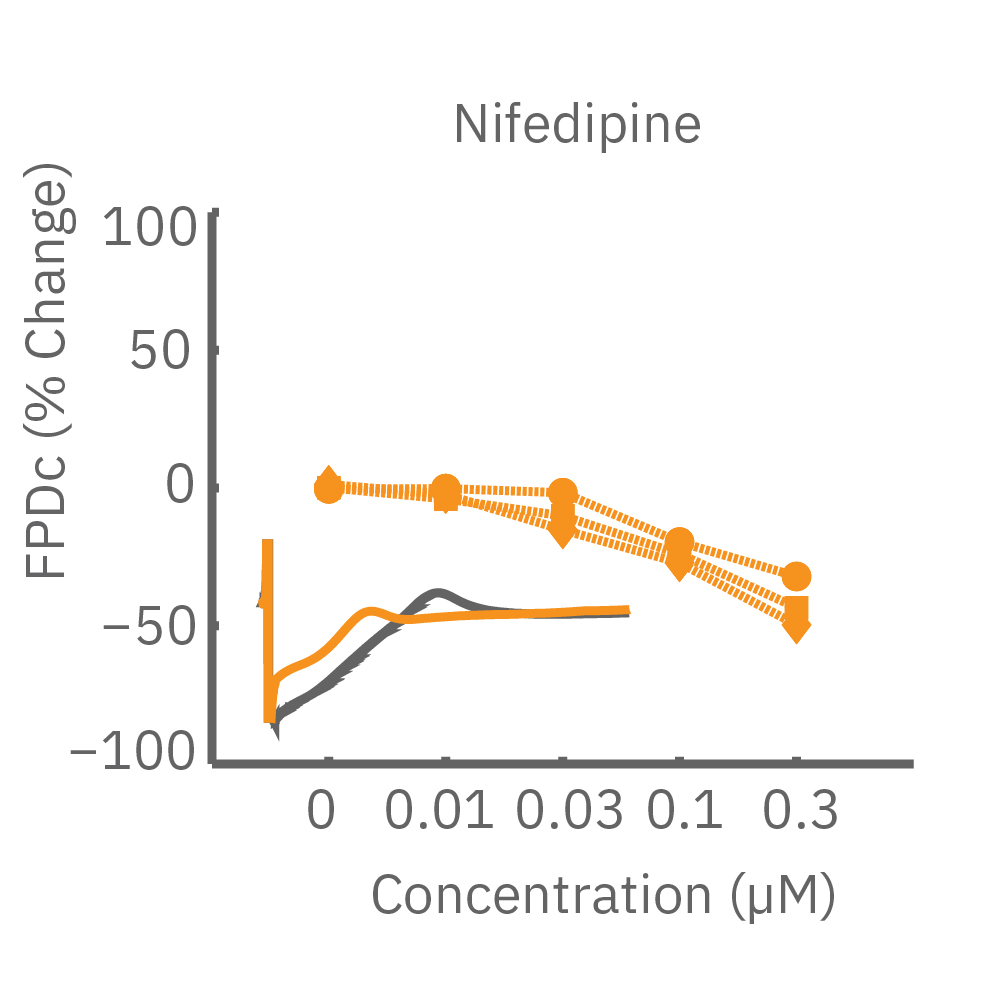
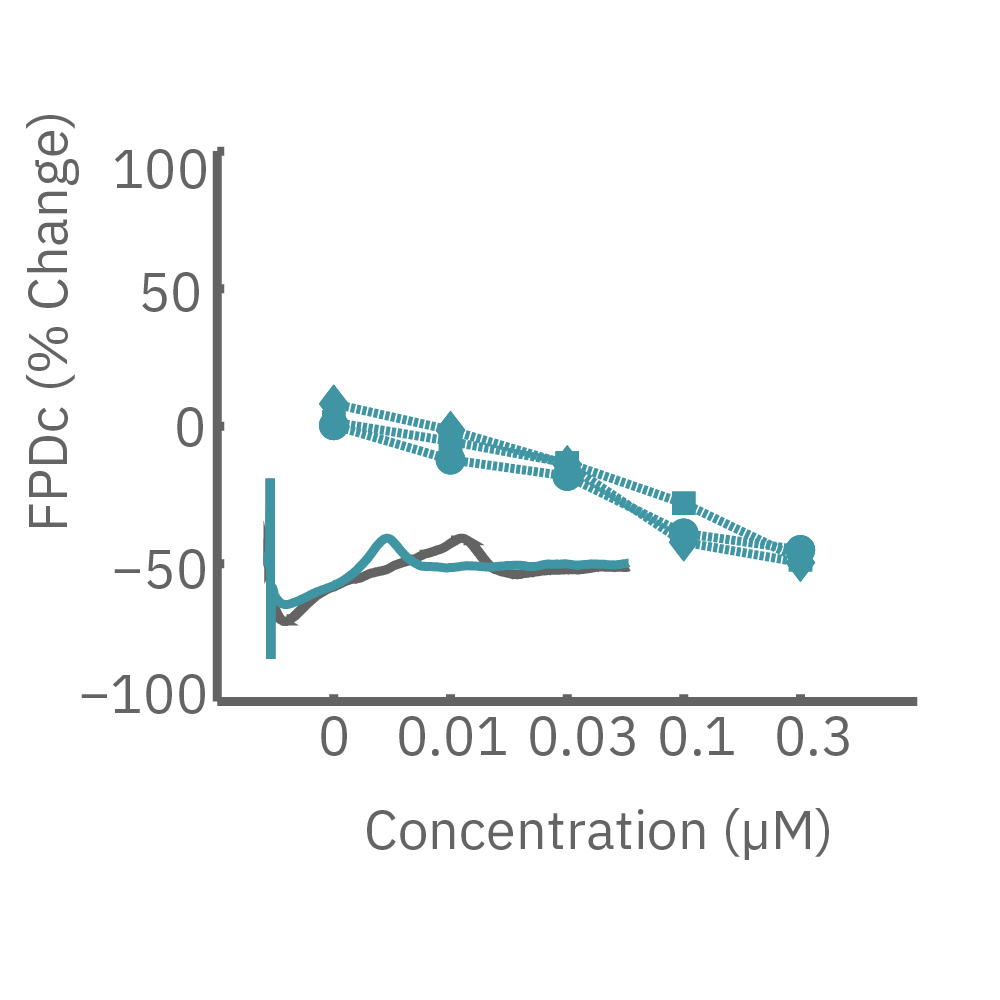
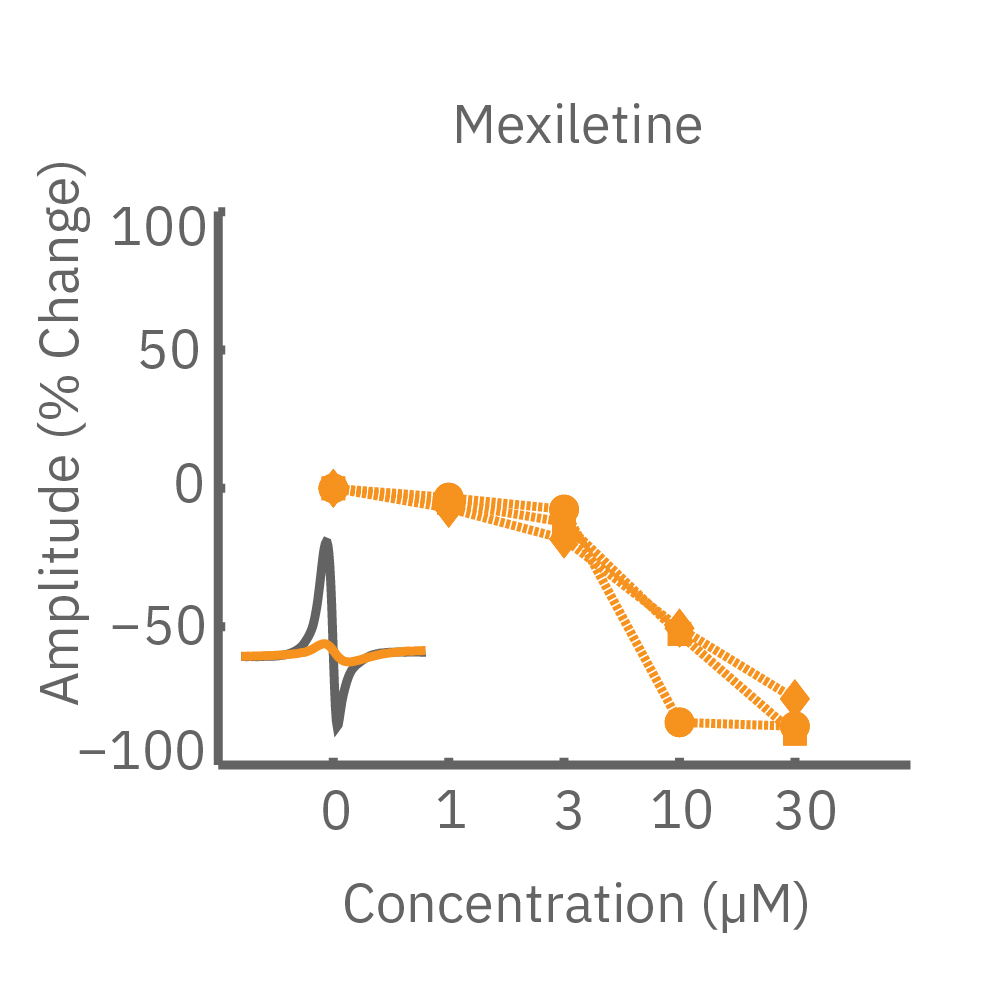
Cross-site reliability of human induced pluripotent stem-cell derived cardiomyocyte based safety assays using microelectrode arrays: Results from a blinded CiPA Pilot Study
Author:
D. Millard, Q. Dang, H. Shi, X. Zhang, C. Strock, U. Kraushaar, H. Zeng, P. Levesque, H. Lu, J. Guillon, J. C. Wu, Y. Li, G. Luerman, B. Anson, L. Guo, M. Clements, Y. A. Abassi, J. Ross, J. Pierson, and G. Gintant
Product:
Maestro Pro,
Maestro Edge,
心筋モジュール,